Disc Lesion and related disorders:
The intervertebral disk: Is composed of two layers: the annulus fibrosus and the nucleus pulposus. The outer, tough layer is the annulus fibrosus which is composed of fibrocartilagenous rings. Typically the outer third of the annulus fibrosus is innervated by the sinuvertebral nerve; diseased disks tend to have deeper innervations. The inner, gelatinous portion of the disk is the nucleus fibrosus and has high water content, but no innervations. The nucleus pulposus is located slightly posterior to the center and changes shape and location based on different types of movement.
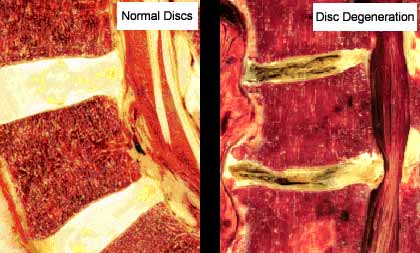
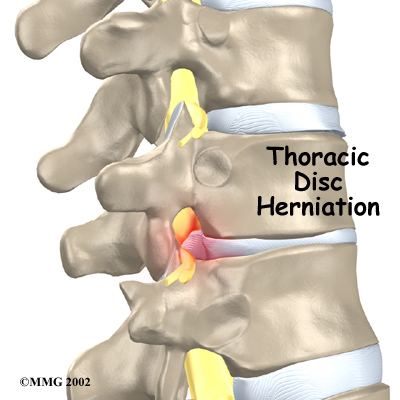
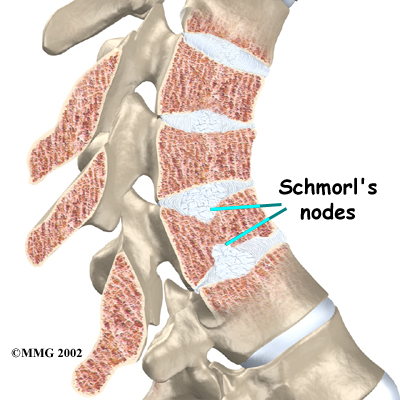
Thoracic Disk Lesions: Disk lesions have been documented at all levels in the thoracic spine, although they are more commonly found in the lower thoracic levels. The major risk factor for thoracic disk herniation is degenerative changes in the disk itself with or without a diagnosis of degenerative disk disease (DDD). It is important to note that due to the anatomical positions of the spinal nerve roots facing inferior-posterior it is less common for a herniation to cause nerve root compressions in the thoracic spine. A disk herniation that protrudes superior or inferior through the vertebral end plate it is referred to as a Schmorl’s node.(Dar, Masharawi et al. 2010) The thoracic spine can be divided up based on anatomical features of the spine and disks. The groups include; T1-T2, T2-T3, T3-T8, and T9-T11. (Dutton 2008)
Demographics:
Incidence/ epidemiology: Thoracic disk herniations are reported to make up on .25-.75% of all disk herniations.(Brown, Deffer et al. 1992)
Clinical Presentation: Clinical manifestations of thoracic disk herniations are variable and vague. This may cause long delays between presentation and diagnosis.
DDX:
Bottom Line: It is reported that as high as 77% of patients with thoracic disk lesion will improve with conservative physical therapy and time.(Brown, Deffer et al. 1992) MRI imaging is still the gold standard diagnostic tool to confirm disk lesions.(Brown, Deffer et al. 1992) If more serious conditions have been ruled out and no red flags are apparent, then conservative treatment is recommended. If patient does not improve with a few treatments or pain is not centralizing a referral should be made full further imaging and diagnostic assessments.
Please refer to the "Disk Lesion and other related disorders" section of the reference list.
Thoracic Disk Lesions: Disk lesions have been documented at all levels in the thoracic spine, although they are more commonly found in the lower thoracic levels. The major risk factor for thoracic disk herniation is degenerative changes in the disk itself with or without a diagnosis of degenerative disk disease (DDD). It is important to note that due to the anatomical positions of the spinal nerve roots facing inferior-posterior it is less common for a herniation to cause nerve root compressions in the thoracic spine. A disk herniation that protrudes superior or inferior through the vertebral end plate it is referred to as a Schmorl’s node.(Dar, Masharawi et al. 2010) The thoracic spine can be divided up based on anatomical features of the spine and disks. The groups include; T1-T2, T2-T3, T3-T8, and T9-T11. (Dutton 2008)
Demographics:
Incidence/ epidemiology: Thoracic disk herniations are reported to make up on .25-.75% of all disk herniations.(Brown, Deffer et al. 1992)
- T1-T2- herniations at this level are very rare.(Kumar and Buckley 1986)
- T2-T3- herniations at this level are the most rare.(Kumar and Cowie 1992)
- T3-T8- herniations at this level are the second most common(Dutton 2008)
- T9-T11- herniations at this level are the most common in the thoracic spine.
- Schmorl’s node- Although Schmorl’s nodes are a common in the normal adult population, their prevalence is controversial and etiology still debatable. Occurs more often in the aging spine as degeneration occurs, but can be seen in the young especially those with conditions such as Scheuermann’s disease.(Dar, Masharawi et al. 2010)
- DDD- Generally a normal process of ageing but when accompanied by pain or chronic pain an actual diagnosis is made of degenerative disk disease. More commonly occurs in lumbar spine but lower thoracic spine is also at risk.
Clinical Presentation: Clinical manifestations of thoracic disk herniations are variable and vague. This may cause long delays between presentation and diagnosis.
- T1-T2- compression of the nerve at this level may result in numbness, tingling, and weakness in the hand, arm, or forearm.(Kumar and Buckley 1986)
- T2-T3- symptoms include referred pain to clavicle, scapular spine, and down the inner arm.(Kumar and Cowie 1992)
- T3-T8- symptoms include referred pain to front, side, or back of trunk. Most often unilateral pain. Compression of the dura at this level can refer pain to neck, mid back extending to the waist line. Patient may complain of a band or belt like pain radiating bilaterally or unilaterally around the trunk.(Dutton 2008)
- T9-T11- At this level it is hard to differentiate between thoracic discs versus upper lumbar disk herniations. Pain referral is usually unilateral radiculopathy to or past the buttock. Patient may complain of a band or belt like pain radiating bilaterally or unilaterally around the trunk.(Brown, Deffer et al. 1992)
- Schmorl’s node- Presentation can be symptomatic or asymptomatic. Patient may have lifelong history of back problems. Schmorl's can occur at multiple vertebrae, and have been found in patients with, chronic pain, radiculopathy, arthritis, scoliosis, stenosis, sports or other injury, or disability. There is much controversy as to a nodes contribution to pain.(Dar, Masharawi et al. 2010)
- DDD- The presentation will vary depending on the severity, but can include the following; idiopathic low back pain, lower thoracic or lumbar radiculopathy, myelopathy, stenosis, Spondylosis, or osteoarthritis.
DDX:
- It is also important to differentiate various spinal conditions from other severe conditions such as metastatic cancer, fracture, infection, and rheumatologic disorders.
- Thoracic disk have been reported to mimic spinal cord tumors.(Bose 2003)
- Thoracic spine herniations will generally not present with classic radiculopathy as in the cervical or lumbar spine. It is important then to rule out conditions prior to confirming a thoracic disk lesion.
- Brown Sequard Syndrome may occur with idiopathic spinal cord herniation. Patient may report band-shaped numbness along a related dermatome; presence of pins and needles sensation in one or both feet, may prefer sleeping sitting up, and pain that has come on gradually over a period of months and felt mainly at night. Pain is uninfluenced by activities.
- Special test and physical exam may include: A thorough neurological screen along with these test; Lhermitte’s symptoms and Hoffman’s - to rule out cervical spine cord referral or Cloward’s points, the slump test to assess neurodynamic mobility.
- If patients present with constitution symptoms (fever, diaphoresis, nausea, vomiting, diarrhea, pallor, dizziness/syncope, fatigue, and weight loss) they should be referred on to physcian.(Boissonnault and Bass 1990)
Bottom Line: It is reported that as high as 77% of patients with thoracic disk lesion will improve with conservative physical therapy and time.(Brown, Deffer et al. 1992) MRI imaging is still the gold standard diagnostic tool to confirm disk lesions.(Brown, Deffer et al. 1992) If more serious conditions have been ruled out and no red flags are apparent, then conservative treatment is recommended. If patient does not improve with a few treatments or pain is not centralizing a referral should be made full further imaging and diagnostic assessments.
Please refer to the "Disk Lesion and other related disorders" section of the reference list.
