Spinal Tumor or Metastasis to the Spine
www.oncolink.org
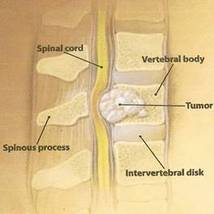
Pathology: Spinal tumor can result from abnormal cell growth in the spinal cord or the vertebral column. Cancer may also metastasize to the spine from an already existing cancer in the body.
"In anyone with a known cancer, the onset of back pain could suggest spinal metastases. An insidious onset of waist level or mid-back pain that becomes progressively more severe and more persistent often occurs. The pain is usually unrelieved by lying down and frequently becomes worse at night. Unexplained weight loss with severe back pain aggravated by rest may point to metastatic carcinoma of the spine. Other bone-related cancers such as multiple myeloma can cause severe, unremitting backaches that are present at rest and become worse when lying down" (Goodman & Snider, 2007).
Demographics:
Incidence: Spinal metastasis only occurs in about 5% of cancer patients (ABTA, 1993). Most common tumors to metastasize to the spine are prostate, lung, and breast cancers (Goodman & Snider, 2007) (Connell, 2009).
Spinal tumors are most common in young and middle aged adults. Sixty percent of all spinal tumors are found in the thoracic region (American Brain Tumor Association (ABTA), 1993) (Goodman & Snider, 2007). This may be because of the length of the thoracic region and its proximity to the mediastinum. These tumors typically are extra-dural and grow outside of the dura mater, but inside the spinal column causing compression of the spinal nerves in that region (ABTA, 1993).
Clinical Presentation (Goodman & Snider, 2007):
Signs & Symptoms:
Tumors that involve the nerve roots will cause motor (weakness, fatigue, spasticity, exaggerated deep tendon reflexes and positive babinski reflex) and sensory (numbness and tingling) dysfunction related to the nerves involved.
Pain may be aggravated by lying down, weight bearing, bending, sneezing or coughing. This pain may be sharp, shooting, deep, or burning pain.
Differential Diagnosis:
Screening questions associated with increased risk of cancer (Deyo, R., 1988):
Need to rule in/out (Connell, 2009):
Bottom Line: Refer Out
If cancer is suspected, the patient needs an immediate referral to their physician. A physical therapist cannot treat the spinal tumor itself. A physical therapist may however treat a patient for musculoskeletal impairments even if they have cancer. Cancer is a contraindication for many modalities and treatment. Contraindicated treatments should not be used throughout treatment of a patient with cancer. Physical therapy may be appropriate after surgical tumor removal. Precautions still need to be taken even after the tumor is removed.
To refer to the references used in compiling this page, please refer to the "Cancer" section in the references list.
"In anyone with a known cancer, the onset of back pain could suggest spinal metastases. An insidious onset of waist level or mid-back pain that becomes progressively more severe and more persistent often occurs. The pain is usually unrelieved by lying down and frequently becomes worse at night. Unexplained weight loss with severe back pain aggravated by rest may point to metastatic carcinoma of the spine. Other bone-related cancers such as multiple myeloma can cause severe, unremitting backaches that are present at rest and become worse when lying down" (Goodman & Snider, 2007).
Demographics:
Incidence: Spinal metastasis only occurs in about 5% of cancer patients (ABTA, 1993). Most common tumors to metastasize to the spine are prostate, lung, and breast cancers (Goodman & Snider, 2007) (Connell, 2009).
Spinal tumors are most common in young and middle aged adults. Sixty percent of all spinal tumors are found in the thoracic region (American Brain Tumor Association (ABTA), 1993) (Goodman & Snider, 2007). This may be because of the length of the thoracic region and its proximity to the mediastinum. These tumors typically are extra-dural and grow outside of the dura mater, but inside the spinal column causing compression of the spinal nerves in that region (ABTA, 1993).
Clinical Presentation (Goodman & Snider, 2007):
Signs & Symptoms:
- Pain
- Decreased sensation
- Spastic muscle weakness
- Progressive muscle weakness
- Muscle Atrophy
- Paraplegia or quadriplegia
- Thoracolumbar pain
- Unilateral groin or leg pain
- Pain at rest and/or night pain
- Bowel/bladder dysfunction (late finding)
Tumors that involve the nerve roots will cause motor (weakness, fatigue, spasticity, exaggerated deep tendon reflexes and positive babinski reflex) and sensory (numbness and tingling) dysfunction related to the nerves involved.
Pain may be aggravated by lying down, weight bearing, bending, sneezing or coughing. This pain may be sharp, shooting, deep, or burning pain.
Differential Diagnosis:
Screening questions associated with increased risk of cancer (Deyo, R., 1988):
- Past history of cancer*
- Age > 50* or <20 years
- Recent, unexplained weight loss*
- Failure of conservative management*
- No relief with complete bed rest *
- Severe pain unaffected by posture or position
- Night pain disturbing sleep
Need to rule in/out (Connell, 2009):
- Multiple sclerosis
- Amyotrophic lateral sclerosis (ALS)
- Herniated disk
- Syringomyelia
- Cauda equina syndrome
- Spinal stenosis
- Ankylosing spondylitis
- Rheumatoid arthritis
- Herniation of nucleus pulposus (pain worse with activity)
Bottom Line: Refer Out
If cancer is suspected, the patient needs an immediate referral to their physician. A physical therapist cannot treat the spinal tumor itself. A physical therapist may however treat a patient for musculoskeletal impairments even if they have cancer. Cancer is a contraindication for many modalities and treatment. Contraindicated treatments should not be used throughout treatment of a patient with cancer. Physical therapy may be appropriate after surgical tumor removal. Precautions still need to be taken even after the tumor is removed.
To refer to the references used in compiling this page, please refer to the "Cancer" section in the references list.